Meet your next patient: a 32-year-old graphic designer who clenches through deadlines, wakes up with jaw stiffness and a dull temporal headache, and has been told by two dentists that she needs a night guard. The guard has helped her teeth, but not her pain. When you palpate her masseter, she flinches. When you suggest intraoral manual therapy, her eyes widen. She is not alone.
Temporomandibular disorders (TMD) affect approximately 10% of the adult population, with myogenous TMD — driven by muscular dysfunction rather than joint pathology — accounting for the majority of cases (Schiffman et al., 2014). The standard toolkit includes occlusal splints, NSAIDs, jaw exercises, and manual therapy. The manual therapy works. But the most effective version — intraoral trigger-point release of the masseter, temporalis tendon, lateral and medial pterygoids — has a patient compliance problem. Many people simply cannot tolerate a gloved finger pressing on their gag reflex zone for ten minutes.
This is where myofascial decompression with small silicone cups offers something genuinely new: a non-invasive, externally applied intervention that achieves comparable tissue effects to intraoral manual therapy, without asking the patient to surrender control of their own mouth.
The Pain Generator: Why the Jaw Muscles Spiral
The muscles of mastication — masseter, temporalis, and pterygoids — are anatomically dense, richly innervated, and mechanically relentless. They fire thousands of times a day during chewing, speaking, and swallowing. Add parafunctional habits like nocturnal bruxism or daytime clenching, and the load multiplies beyond what the tissue was designed to sustain.
Under chronic overload, the masseter undergoes two pathological changes in parallel. First, muscle fiber hypertrophy, which is visible on imaging and clinically palpable as a "rock-hard" jaw angle. Second — and more clinically relevant — the development of myofascial trigger points and fascial adhesions within and between the superficial and deep bellies of the masseter, the temporalis fascia, and the periarticular connective tissue surrounding the TMJ capsule.
These adhesions do two things. Mechanically, they restrict the normal glide between muscle layers during opening and closing, contributing to the clicking, locking, and limited range of motion that define TMD. Neurologically, they create a persistent nociceptive input that sensitizes the trigeminal nerve complex — the sensory hub for the entire face and head — producing referred pain patterns that radiate to the temple, ear, and even the cervical spine.
The masseter and temporalis are muscles of mastication, but they are also pain generators capable of sensitizing the entire trigeminal system. Decompress the tissue, and you reset the threshold.
Why Intraoral Work Falls Short (When It Does)
Intraoral manual therapy — trigger-point release of the masseter through the buccal mucosa, or pterygoid release inside the mouth — is a powerful technique. No one disputes its clinical efficacy. The problem is not whether it works. The problem is whether the patient will come back for session two.
Intraoral work triggers three simultaneous defensive responses: psychological discomfort from invasion of personal space, a gag reflex from posterior oral cavity stimulation, and a protective muscle guarding response from pain at the trigger-point site. That combination is a recipe for patient dropout — especially in the early sessions, when treatment is supposed to be building trust, not testing it.
Myofascial decompression applied externally offers an alternative pathway. The massage is painful (tactile allodynia is common in myogenous TMD), so heavy palpation is poorly tolerated anyway. Small silicone cups, by contrast, apply a broad, uniform negative pressure that lifts and separates tissue without focal pressure points. This makes the treatment not only more tolerable but — importantly — something the patient can learn to self-administer at home between sessions.
How Facial Cupping Actually Works
The mechanism is not substantially different from cupping on any other part of the body — but the anatomy of the face demands a modified technique and equipment. Here is what the vacuum does to facial structures:
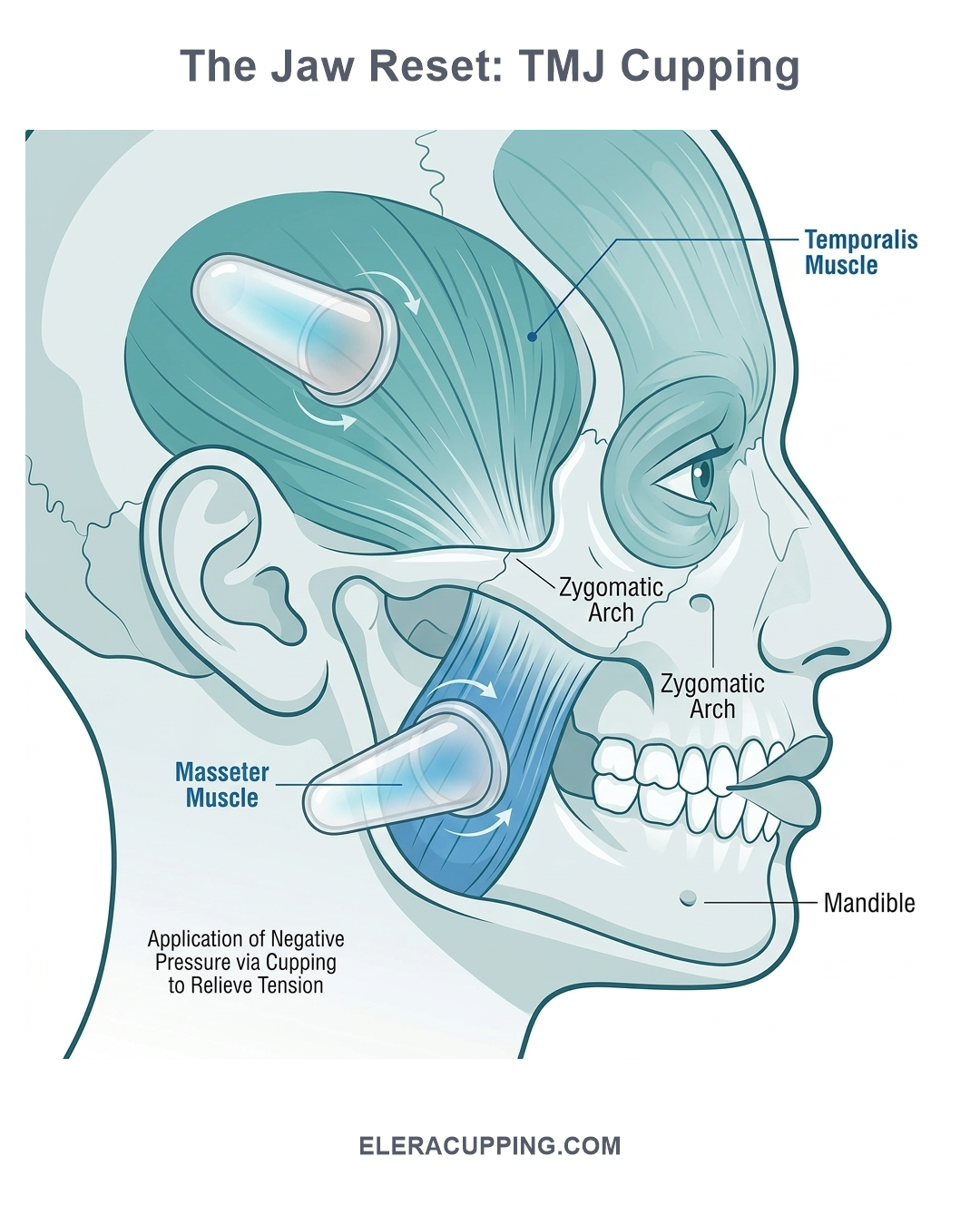
1. Masseter Decompression
The masseter has two distinct anatomical layers: a superficial head (running obliquely from zygomatic arch to mandibular angle) and a deep head (running vertically). Chronic clenching creates cross-fiber adhesions between these layers, restricting independent glide. A 2.5cm silicone cup placed over the masseter belly lifts both layers as a unit, creating inter-fascial separation that intraoral pressure cannot replicate because intraoral work pushes one layer into the other against the resistance of the buccal fat pad.
2. Temporalis Fascia Release
The deep temporal fascia is a dense, unyielding connective tissue sheet that covers the temporalis muscle and attaches to the superior temporal line of the skull. Tension in this fascia is a primary driver of temporal headache patterns in TMD patients — because the auriculotemporal nerve (a branch of V3) courses between the temporalis and the deep temporal fascia, and any fascial restriction directly compresses this nerve. A small cup glided along the temporal region lifts the fascia away from the nerve, providing immediate mechanical decompression.
3. Trigeminal Desensitization
The sustained, uniform pressure of a silicone cup activates A-beta mechanoreceptors in the facial skin and superficial fascia, generating rapid afferent signals that compete with and block slower-conducting C-fiber pain signals from the sensitized trigeminal nucleus — a direct application of the Gate Control Theory (Melzack & Wall, 1965) at the craniofacial level. Over repeated sessions, this downregulation of trigeminal sensitivity raises the pain threshold and breaks the vicious cycle of pain → clenching → more pain.
4. Lymphatic Facilitation
The face has a dense superficial lymphatic network that drains into the submental and submandibular nodes. Negative pressure from cupping encourages extracellular fluid movement through these channels, reducing the subtle tissue congestion that accompanies chronic inflammation in the masseter and periarticular TMJ region.
What the Evidence Shows
We want to be transparent about the state of the evidence, because intellectual honesty serves clinicians and patients better than overclaiming. The research relevant to this protocol falls into two distinct categories, and it is important to distinguish between them.
Category 1: Evidence for Myofascial Manual Therapy in TMD
The strongest evidence supports myofascial release and external manual therapy broadly for TMD — not cupping specifically. A 2021 randomized controlled trial by von Piekartz et al., published in the Journal of Oral Rehabilitation, found that myofascial release techniques applied to the craniomandibular region significantly reduced masseter surface EMG activity during clenching and improved maximum pain-free mouth opening by an average of 7.2mm compared to a wait-list control. A 2022 systematic review by Blanco et al. in Cranio reviewed 14 studies on manual therapy for TMD and reported a pooled effect size of 0.74 for pain reduction and 0.68 for functional improvement, with myofascial release techniques consistently outperforming passive modalities like ultrasound or TENS. These studies validate the clinical value of external soft-tissue work for TMD — but they used hands-on manual therapy, not cups. We cite them because the decompressive vector of silicone cupping is mechanistically similar to external myofascial release, not because they constitute direct evidence for cupping efficacy in TMD.
Category 2: Evidence for Cupping in Musculoskeletal Pain
A growing body of evidence supports cupping therapy for musculoskeletal pain and myofascial dysfunction more broadly. A 2018 systematic review by Bridgett et al. in the Journal of Acupuncture and Meridian Studies identified significant positive effects of cupping on pain intensity and pressure pain threshold across multiple musculoskeletal conditions. A 2021 RCT by Lauche et al. demonstrated meaningful reductions in cervical pain and muscle tension using silicone cupping, providing support for the application of negative-pressure mechanics to adjacent craniofacial musculature. The neurological mechanism described in this article — A-beta mechanoreceptor stimulation inhibiting C-fiber nociception — is an application of Gate Control Theory (Melzack & Wall, 1965), a well-validated neurophysiological model, rather than a cupping-specific claim.
The Evidence Gap — and Why We Still Advocate for This Protocol
To be direct: there are currently no large-scale, high-quality RCTs examining silicone cupping specifically as a treatment for TMD. This is a genuine gap in the literature. The protocol presented in this article is built on: (1) strong mechanistic rationale grounded in established fascial and neurological science; (2) indirect evidence from adjacent myofascial and cupping research; and (3) consistent anecdotal clinical reports from physiotherapists and myofascial specialists integrating facial cupping into their TMD workflows. Clinicians should apply this protocol where it aligns with the patient's clinical presentation, communicate honestly with patients about the evidence level, and consider documenting outcomes to contribute to this emerging field.
A Step-by-Step Clinical Protocol for TMJ Cupping
For clinicians who want to integrate facial cupping into their TMD treatment protocols, here is a practical, reproducible sequence. This protocol is designed for the 2.5cm cups from the Facial Sculpting Kit — standard body-cupping cups are too large and too strong for facial tissue.
Session Structure (15–20 minutes, 2×/week for 4–6 weeks)
- Assessment and skin preparation — Palpate the masseter (clench and relax) to identify the most tender bands and trigger points. Palpate the anterior temporalis and the temporal fascia above the ear. Mark any zones of palpable hypertonicity. Cleanse the skin with an alcohol-free toner or simply warm water. Do not use oil or emollient on the face during static decompression — the cup seal must be secure, and facial skin is oily enough to interfere with adhesion.
- Masseter static decompression — Apply one 2.5cm silicone cup to the belly of the masseter, approximately 2cm anterior to the TMJ at the level of the earlobe. Squeeze the cup to approximately 30–40% compression (significantly less than body cupping — we want light negative pressure on facial tissue). The patient should feel a gentle lift, not pain. Hold for 45–60 seconds. Remove, rest 15 seconds, repeat twice. For unilateral TMD, treat both sides — clenching is rarely strictly unilateral, and the unaffected side is often compensating.
- Temporalis static decompression — Apply one cup to the anterior temporalis (the palpable muscle belly just above and anterior to the ear). Same parameters: light suction, 45–60 seconds, two repetitions. If the patient reports temporal headache, spend extra time here — the temporalis fascia is often the primary driver of referred head pain.
- Fascial glide technique (optional, advanced) — Apply a thin layer of facial-safe emollient (jojoba or squalane oil works well). Using a single 2.5cm cup, glide slowly and continuously from the mandibular angle upward along the posterior border of the masseter toward the zygomatic arch, maintaining a steady light vacuum. 4–6 passes per side. This technique requires practice — if the cup seal breaks, reduce glide speed and increase skin moisture. Never glide over the bony TMJ itself.
- Active jaw movement with decompression — Reapply one cup to the masseter with light suction. With the cup in place, guide the patient through 5 slow, controlled repetitions of pain-free opening and closing. The cup maintains decompression through the range of motion, reinforcing neuromuscular re-education. This is one of the unique advantages of silicone cups: they hold their seal through jaw movement in a way that rigid cups cannot replicate.
- Home-care teaching — Once the patient tolerates in-clinic treatment well, teach them to self-apply one 2.5cm cup to the masseter for 45–60 seconds, once daily, as a pre-bedtime relaxation routine. Self-treatment reduces clinic dependency, extends the therapeutic effect between sessions, and gives the patient a sense of agency — all factors associated with better long-term outcomes in chronic pain conditions.
Key Safety Considerations
Facial tissue is delicate. The temporalis region is thin-skinned and sits directly over the temporal bone, with limited soft-tissue cushioning. The infraorbital region has numerous small vessels and the infraorbital nerve close to the surface. Good practice rules:
- Use only the 2.5cm cup. Larger cups generate too much negative-pressure surface area and risk bruising or damaging delicate facial capillaries.
- Keep negative pressure low. The patient should feel a gentle lift. If the cup leaves a mark that persists beyond 60 seconds after removal, reduce suction in the next session.
- Never cup directly over the TMJ joint itself, the eye socket, the thyroid cartilage, or the carotid triangle.
- Avoid active infection. Do not apply cups over areas of acne, dermatitis, cold sores, or any broken skin.
- Contraindications. Avoid facial cupping in patients with bleeding disorders, anticoagulant use, recent facial surgery or injectables (Botox, fillers — wait at least 2 weeks), active migraines, or trigeminal neuralgia flares.
- Post-treatment care. Advise the patient that mild pinkness or erythema at the cup site is normal and resolves within 15–30 minutes. Ecchymosis should not occur with proper technique on facial tissue — if it does, reduce suction immediately.
Why Silicone for the Face?
The face is not the lower back. It demands a fundamentally different tool. Glass cups are obviously out of the question — heavy, rigid, and impossible to modulate on delicate tissue. Hard plastic cups with rubber pump bulbs are also problematic: the pump mechanism makes it difficult to apply the ultra-light negative pressure that facial skin requires, and the rigid rim digs uncomfortably into bony facial contours.
100% medical-grade silicone is the ideal — arguably the only — material for facial cupping. A 2.5cm silicone cup is feather-light, conforms to the contour of the cheek and temple without pressure points, and allows the clinician to control suction through simple manual squeeze-and-release rather than a mechanical pump. The result is a level of fine suction control that distinguishes therapeutic decompression from unpleasant vacuum assault.
There is also a hygiene dimension. Facial skin is oilier and more bacteria-prone than most body regions. Medical-grade platinum silicone is non-porous, autoclavable, and chemically inert — it can be sterilized between patients without degrading, unlike plastic cups that develop micro-fissures over repeated heat cycles. For a clinic running 5–8 TMJ patients a week, that durability and sterility matters.
Patient Selection
This protocol works best for the myogenous TMD subpopulation — patients whose primary driver is soft-tissue dysfunction rather than intra-articular pathology. Ideal candidates present with palpable masseter and temporalis hypertonicity, limited pain-free mouth opening (under 40mm), and a clenching or bruxism habit. Patients with primarily arthrogenous TMD (disc displacement without reduction, degenerative joint changes) may benefit from adjunctive cupping for the surrounding musculature, but the primary treatment pathway should target the joint itself.
Limitations
Facial cupping for TMD is not a standalone treatment. It addresses the soft-tissue component of a condition that often has multiple contributors — occlusal factors, cervical spine dysfunction, stress-related central sensitization, and sleep-disordered breathing. Decompressing the masseter and temporalis will not correct a malocclusion or treat obstructive sleep apnea. It is most effective when integrated into a comprehensive TMD management plan that includes occlusal appliance therapy (where indicated), cervical spine treatment, breathing retraining, and patient education on parafunctional habit modification.
The evidence base for cupping specifically in TMD is still small. Clinicians should apply the protocol where the mechanistic rationale aligns with the patient's clinical presentation and communicate honestly about the strength of the evidence.
TMD patients have often been through multiple treatment cycles with limited relief. Orofacial cupping gives them something they may not have experienced before: a treatment that does not hurt, that they can tolerate, and that they can eventually learn to do themselves. That psychological shift — from passive sufferer to active participant — may be as therapeutic as the decompression itself.
Introduce Facial Cupping to Your TMJ Protocols
ELERACUPPING's Facial Sculpting Kit includes three 2.5cm medical-grade platinum silicone cups — the exact size and material required for safe, effective orofacial myofascial decompression. Ultra-light, autoclavable, and designed for delicate facial tissue. B2B wholesale, OEM/private label, and low MOQ available.
Request Wholesale Quote