Every clinician knows this patient: a 38-year-old who spends eight hours a day at a desk, has done months of physical therapy, stretches every morning, and still wakes up with lower back stiffness that only gets worse as the day wears on. They have been told their glutes are weak, their hamstrings are tight, and their core needs more work. They have done the exercises. The pain always comes back.
Why? Because the standard lower back rehab checklist—strengthen, stretch, stabilize—operates on an incomplete model of what drives chronic low back pain (CLBP). The muscles matter. The discs matter. But there is a structure that sits between all of them, and when it gets stuck, nothing else works properly.
The thoracolumbar fascia (TLF) is the largest and most densely innervated fascial structure in the human body. It is also the most ignored contributor to persistent lower back pain.
The Fascial Blind Spot
The TLF is a multi-layered sheath of dense connective tissue that wraps the lower back like a natural weightlifter's belt. Its posterior layer spans from the thoracic spine down to the sacrum, connecting the latissimus dorsi, gluteus maximus, and paraspinal muscles into a continuous force-transmission network.
Here is what most clinicians do not realize: the TLF is richly innervated with free nerve endings—nociceptors that are perfectly capable of generating back pain independently of any muscle strain or disc pathology. Landmark studies by researchers like Schilder et al. in the journal Pain demonstrated that injecting hypertonic saline into the TLF of healthy subjects produced pain patterns nearly identical to those reported by patients with chronic LBP. The tissue itself can hurt—not just the structures underneath it.
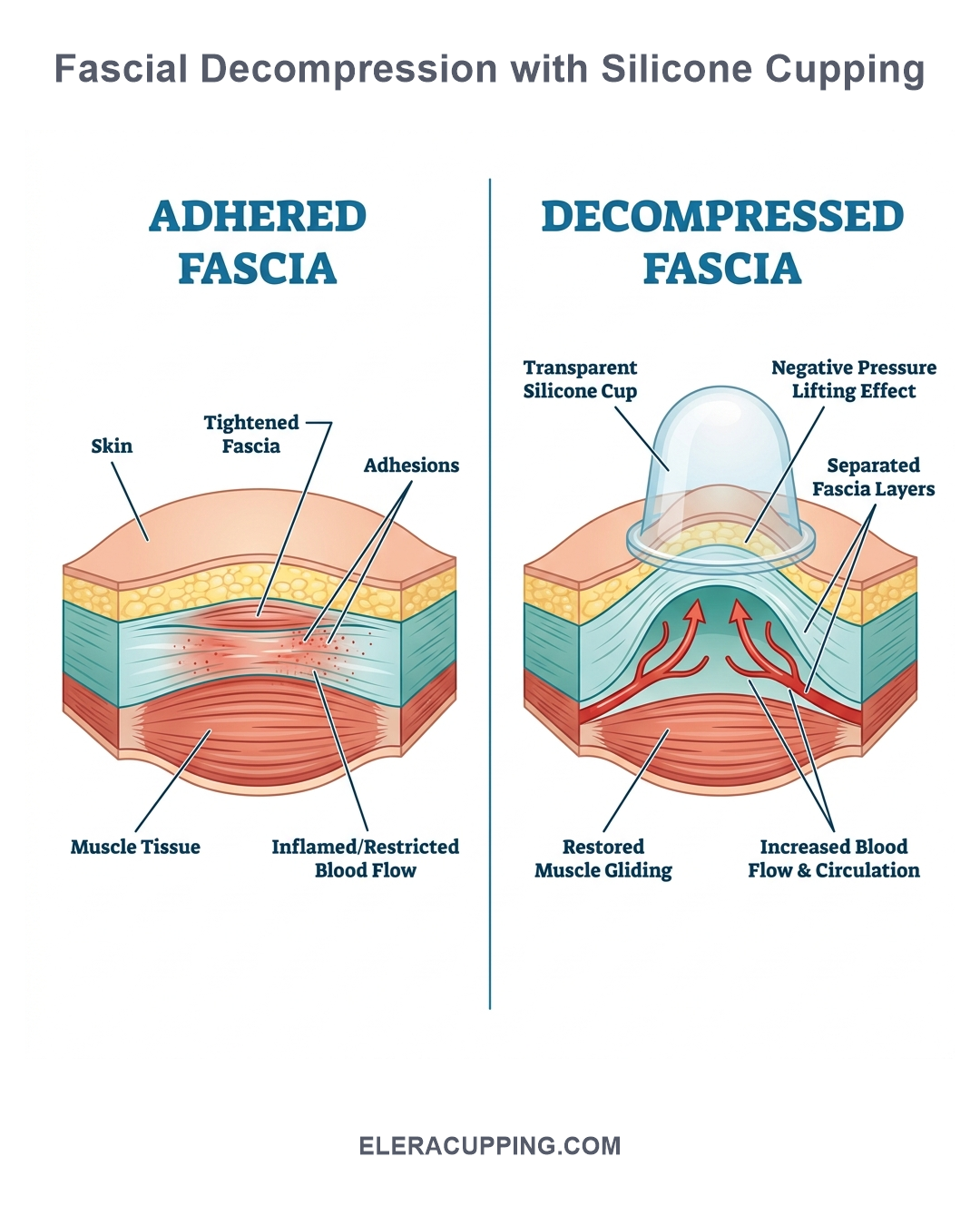
When the TLF becomes chronically adhered—through prolonged sitting, repetitive microtrauma, or insufficient movement variability—the normal glide between its layers is lost. This adhesion compresses and irritates the embedded nociceptors with every spinal movement. The result is persistent, activity-dependent pain that does not resolve with stretching (which cannot pull adhered layers apart) or strengthening (which increases compressive load through the same stuck tissue).
The thoracolumbar fascia is not passive wrapping. It is a densely innervated sensory organ capable of generating and sustaining chronic low back pain independent of muscles, discs, or joints.
Why Standard Approaches Fall Short
To understand why CLBP recurs, consider the biomechanics of the TLF during a basic movement: bending forward to tie your shoes. In a healthy spine, the posterior TLF layers slide freely over the underlying erector spinae as the lumbar spine flexes. This sliding motion distributes tensile load evenly across the lower back and signals normal movement to the nervous system.
In a spine with adhered TLF, that sliding does not happen. The fascia remains tethered to the muscle beneath it. Each forward flexion tugs directly on the adhered nociceptors, triggering pain signals before any muscle or disc is even stressed. The patient interprets this as "my back is tight" and responds with more stretching—which, unfortunately, cannot break a fascial adhesion because stretching only applies longitudinal tension, not vertical separation.
This is the mechanical trap that keeps CLBP patients cycling through failed treatments: the tissue needs to be lifted apart, not pulled longer.
How Myofascial Decompression Breaks the Cycle
Myofascial decompression (cupping therapy) addresses the adhered TLF through a mechanism that neither stretching nor strengthening can replicate: negative pressure separation.
When a silicone cup is applied over the lumbar paraspinal region, the vacuum lifts the posterior TLF layer away from the underlying muscle fascia. This vertical separation achieves three distinct therapeutic effects:
1. Mechanical Separation
The lift restores inter-fascial glide immediately. By physically separating the adhered layers, the vacuum breaks the mechanical tether that was irritating the TLF nociceptors. Patients often report a sensation of "space" or "release" in the lower back within seconds of cup application—distinct from the discomfort of deep tissue massage.
2. Mechanotransduction and Tissue Remodeling
The tensile strain on TLF fibroblasts triggers cellular signaling cascades (FAK, MAPK pathways) that downregulate pro-inflammatory cytokines like TNF-alpha and upregulate matrix metalloproteinases (MMPs) responsible for remodeling dysfunctional extracellular matrix. This is not just temporary pain relief—it is a genuine shift in the tissue's structural environment.
3. Neuromodulation via the Pain Gate
The broad, uniform vacuum activates A-beta mechanoreceptors embedded in the TLF, generating rapid afferent signals that compete with and block slower-conducting C-fiber pain signals at the dorsal horn—a direct application of the Gate Control Theory of Pain (Melzack & Wall, 1965). Simultaneously, the rhythmic stimulation of paraspinal fascia during gliding techniques increases parasympathetic vagal tone, shifting the nervous system out of the chronic sympathetic drive that characterizes persistent pain states.
What the Evidence Shows
Recent systematic reviews and meta-analyses published in peer-reviewed journals have examined randomized controlled trials comparing cupping therapy to usual care for chronic low back pain. The pooled analyses consistently find statistically significant reductions in pain intensity and improvements in functional disability at follow-up, suggesting that fascial decompression is a highly effective adjunct to standard care.
Furthermore, controlled clinical studies comparing active cupping (using silicone cups) to conventional physiotherapy for CLBP often report significantly greater improvements in both disability indexes and pressure pain thresholds over the lumbar spine. The critical advantage noted is the ability for patients to perform active lumbar range of motion while the cups are in place—a capability unique to elastic silicone cups that rigid glass or plastic cannot replicate.
A Clinical Protocol for Lumbar Cupping
For clinicians interested in integrating TLF decompression into their LBP protocols, here is a practical sequence:
- Positional assessment — Identify the region of greatest fascial restriction through skin rolling and passive flexion/extension testing. The most common restriction pattern is bilateral paraspinal TLF tightness from T10 to L5.
- Static decompression — Apply 2–4 silicone cups paraspinally over the restricted region. Use an XL or L Classic Mushroom cup for the lumbar area. Leave static for 2–3 minutes to allow the vacuum to establish mechanical separation.
- Dynamic gliding — Apply a light emollient and glide the cups longitudinally along the paraspinal region from the lower thoracic to the sacral area, maintaining vacuum throughout. 5–8 passes per side.
- Active movement with cups — Keep 2 cups in place on the most restricted segments and guide the patient through active lumbar flexion, extension, and lateral flexion. The cups maintain decompression through the full range, reinforcing neuromuscular re-education.
- Home self-care — Teach the patient to apply one XL silicone cup to the most restricted paraspinal region for 2–3 minutes as a daily pre-exercise warm-up, extending the therapeutic effect between sessions.
Why Silicone Matters for the Lumbar Spine
The lumbar spine presents a unique challenge for cupping: it is highly mobile, heavily muscled, and curved. Rigid glass cups cannot maintain seal during active lumbar movement because the edge lifts as the spine extends or flexes. Hard plastic cups dig into the paraspinal muscles when the patient moves, triggering a protective contraction that undermines the decompression.
100% medical-grade silicone is the only material that solves these problems. The elasticity of a premium silicone cup—like the Classic Mushroom design—allows it to elongate and conform to the changing contour of the lumbar spine during flexion and extension. The soft edges distribute the vacuum evenly across the paraspinal tissue without pressure points. The seal holds through a full squat, a forward bend, or a seated rotation.
There is also a hygiene advantage for clinic use: medical-grade platinum silicone is autoclavable, chemically inert, and resistant to surface degradation. Unlike hard plastic cups that develop micro-cracks over repeated sterilization cycles—creating crevices for bacterial biofilm—silicone cups maintain their integrity through hundreds of treatment sessions.
Limitations
Cupping is not a replacement for a comprehensive LBP rehabilitation program that includes appropriate loading, movement retraining, and patient education. Fascial decompression addresses the tissue-level restriction that standard approaches miss, but it works best as part of a multimodal strategy. The evidence base for cupping in CLBP is growing but still limited by small sample sizes and inherent blinding challenges. Deep, isolated paraspinal trigger points may still respond better to dry needling or manual therapy in some patients.
Lower back pain is rarely caused by a single structure. But when standard rehab plateau—when stretching and strengthening stop producing results—the adhered thoracolumbar fascia is often the missing piece. Myofascial decompression is not a replacement for exercise. It is the tool that makes the exercise work again.
Equip Your Practice with Medical-Grade Silicone Cupping
ELERACUPPING manufactures premium 100% medical-grade silicone cupping sets trusted by sports rehabilitation clinics and SPA distributors worldwide. Our Classic Mushroom XL and L sizes are ideal for lumbar fascial decompression protocols. B2B wholesale, OEM/private label, and low MOQ available.
Request Wholesale Quote